The coronavirus pandemic explained, one year on
We've learned so much about the coronavirus in the more than 365 days since our first guide was published.



On Jan. 19, 2020, CNET posted its first guide to a mystery coronavirus discovered in the Chinese city of Wuhan. Dozens of cases and two deaths had been recorded, but as we wrote at the time, little was known about "how destructive the new virus might be." The coronavirus -- and the disease it causes -- hadn't even been named. It hadn't officially been found in the US.
Today we call the mystery pathogen SARS-CoV-2. It's responsible for COVID-19, a respiratory illness that has infected over 100 million people. In just one year, we've gone from two deaths to 2 million, across the world.
Reading our original article, it's immediately obvious that everyone -- virologists, epidemiologists, journalists -- was flying blind in those very early days. We were oblivious, perhaps even shortsighted. No one predicted exactly what would occur over the next 365 days, though there were those who tried to sound the alarm early.
Back then, research had only just begun to uncover how we might combat COVID-19. In those early days, new data came quickly, but there were significant gaps in our knowledge that allowed a deluge of misinformation, conspiracy and fear to fester.
We attempted to answer six questions on Jan. 19, 2020. They were fundamental questions about the new virus, its symptoms and how it spread. A year on, we are revisiting them. This updated guide reveals how much we've learned and charts how science was able to provide certainty and hope in the face of the biggest public health crisis in a century.
Science and technology have provided clarity where there was none -- but much remains unknown as we face the second pandemic year.
What is a coronavirus?
There is no better-known virus on Earth than the coronavirus, SARS-CoV-2, which was first detected in Wuhan in December 2019. In a landslide victory, the coronavirus beats out Ebola, influenza, HIV and the panoply of viruses that cause the common cold for Earth's Most Renowned Virus. But it's not the only coronavirus.
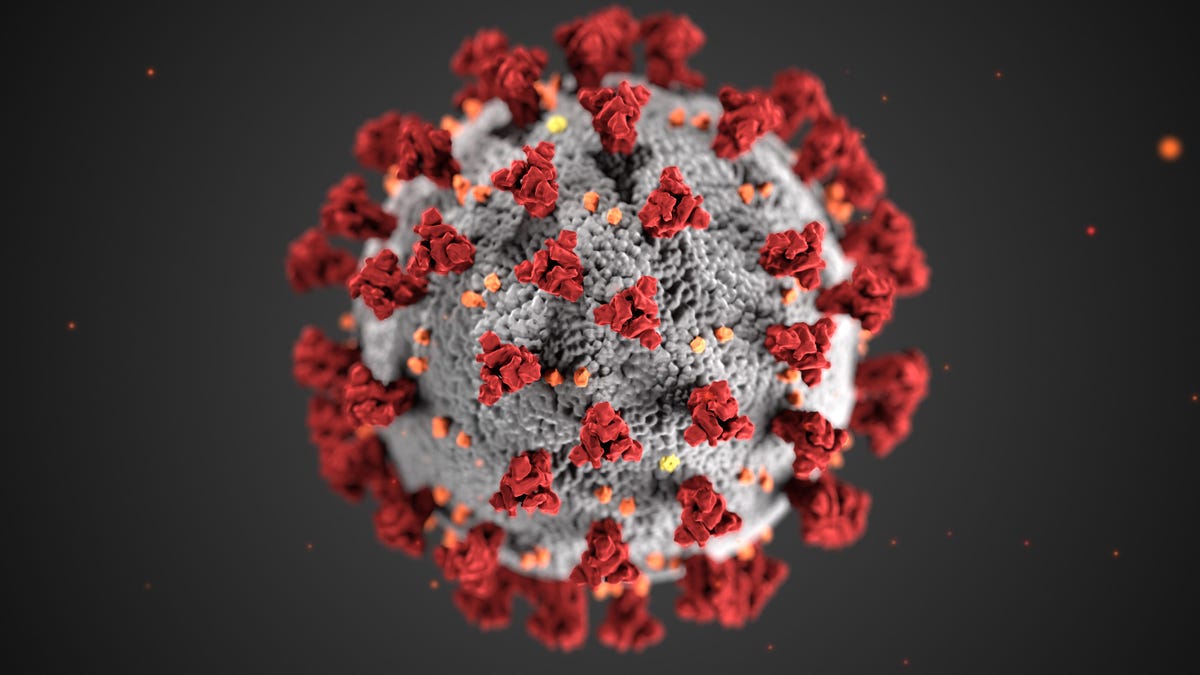
Coronaviruses belong to a taxonomic family known as Coronaviridae, which includes dozens of different species. First described in 1968, coronaviruses are shaped like soccer balls wrapped in a blanket of spikes. Under an electron microscope, these spikes look like the sun's corona -- hence their name. Only a handful are known to cause disease in humans.
World famous.
The SARS epidemic of 2002-03 and the MERS epidemic of 2012 showed coronaviruses have the capability to cause significant outbreaks of deadly disease. The epidemics launched an international effort to understand the pandemic potential of coronaviruses.
In 2020, 65,000 papers were published and listed on PubMed under the term "coronavirus." A year prior, that number was 885. The lessons we're learning about SARS-CoV-2 are relevant to this particular virus but also revealing more and more about coronaviruses in general. "It is the fastest-moving field I have ever seen in my life," says Stuart Turville, an immunovirologist at the Kirby Institute in Australia.
Among the defining characteristics of the coronavirus are the numerous "spikes" on its surface. These proteins function like keys, allowing a coronavirus to enter a cell. Spikes are able to unlock entry by binding to a "lock," a cell surface protein in humans (and other animals) known as ACE2. The two pieces of molecular machinery have been the focus of thousands of researchers around the world since January 2020.
During the SARS epidemic, scientists had learned that the spike elicits an immune response, stimulating cells and antibodies to fight the virus. This gave them a headstart on building vaccines against SARS-CoV-2. "Labs could download the [genetic] sequence of the spike protein and start developing vaccines as soon as the scientists in China had sequenced it," says Larisa Labzin, an immunologist at the University of Queensland, Australia. By the end of 2020, several vaccines had already been rolled out.
But the spike in SARS-CoV-2 appears to be changing.
We're seeing new variants of the virus emerge across the world, with slight changes to the spike proteins. Scientists are watching these changes occur in real time by analyzing the genome of virus samples faster than ever before. We don't yet understand a lot about why they are changing. The virus is evolving in a way that may help it evade our immune system, and similar variants seem to be cropping up across the globe -- a development that may affect vaccines.
Where did the virus come from?
Of the six questions posed in January 2020, this remains the most difficult to answer -- and investigations into the origins of the pandemic have become a tangled mess of conspiracy and politicking.
In our initial report, we said the virus "appears to have originated in the Huanan Seafood Wholesale Market" in Wuhan. A majority of the early cases were linked to the market in December 2019, but further investigation revealed COVID-19 infections in people who had no known contact with the market at all.
The market was shut down on Jan. 1, 2020, and hundreds of environmental samples from the site were analyzed. Traces of SARS-CoV-2 were found, but there was no definitive link between animals in the market and the virus. The World Health Organization and China's CDC have both suggested that the coronavirus may have been circulating in Wuhan prior to the outbreak and that the market merely helped amplify the spread. A year on, we still don't have a clear answer about the market's role in the pandemic.

Bats are reservoirs of coronavirus -- did this pandemic begin in a bat?
Scientists have not yet discovered a direct progenitor to SARS-CoV-2, but they have found several bat coronaviruses that share genetic similarities. One, known as RaTG13, shares 96.2% of its genome with SARS-CoV-2. Another, RmYN02, shares 93.3%. Both highlight how viruses like SARS-CoV-2 can arise in nature. Some scientists argue this shows clear evidence for a natural origin.
But the origin puzzle has not been solved. While natural origin seems likely, an accidental leak from the Wuhan Institute of Virology, scientists say, cannot be dismissed. The so-called "lab leak theory" has become intricately tied to conspiracy theories in the past, but it's important to separate the more extreme, debunked ideas about COVID-19's emergence (it's created by Bill Gates or it's a bioweapon, for instance) from a legitimate investigation into an accidental leak.
In January 2021, a 10-person investigative team convened by the WHO arrived in Wuhan to carry out examinations of the Huanan market by mapping supply chains and testing frozen sewage samples for hints about the virus. The investigation's terms of reference don't mention investigating a lab leak. Some scientists are concerned the investigation doesn't focus on this area of inquiry enough and has a significant conflict of interest. "I have zero confidence left in the WHO team," Alina Chan, a scientist at the Broad Institute of Harvard and MIT, told CNET in January.
How many cases have been reported?
Over 100 million cases have been reported, with COVID-19 infections now found on every continent, including Antarctica. Over 2 million people have died.
Over half of these deaths have happened in just six nations: the US, Brazil, India, Mexico, the UK and Italy. In the US alone, over 400,000 deaths have been recorded.
When the history of the pandemic is written, these nations will be considered failures. Mismanagement, misinformation and misapprehension inhibited an effective response from their governments, leading to uncontrolled spread and overwhelmed health care systems.
Coronavirus updates
On the other end of the scale are great success stories. Australia's and New Zealand's efforts to aggressively suppress or outright eliminate the virus with hard, fast lockdowns and strict border controls have helped to stop outbreaks throughout the year.
In Sydney, life feels like it has settled into a "COVID normal" -- the ubiquity of face masks at the supermarket and on public transport, and the need to sign in with a QR code at every venue we visit, is a reminder that the virus still poses a serious threat. Complacency crept in, particularly over the holiday period, but outbreaks are dealt with swiftly and lockdowns are mandated as soon as cases begin to spike. There's been a wide public acknowledgement and acceptance that the situation changes daily -- we've had to adapt to that in order to prevent the virus from spreading uncontrollably.
How does the coronavirus spread?
We did not have the answer to this question on Jan. 19, 2020. Initially, there were limited reports of health officials and health care workers being infected. With only 60 known cases, it seemed SARS-CoV-2 was not highly contagious. We now know that was wrong.
Scientists understood from early on that the virus predominantly spread through the air, moving from person to person via coughing, sneezing and talking. Such expulsions would produce large droplets ferrying viral particles between people. This idea informed early attempts to slow down the virus, focusing on social distancing, because large droplets do not carry far.
But some scientists were convinced that large droplets were not the only form of transmission for COVID-19. Perhaps small droplets -- aerosols, as they're known -- were also contributing to the spread. Because of their size, these droplets spent a lot longer in the air and may accumulate over time. This led to heated discussion around the airborne transmission of SARS-CoV-2.
The debate came to a head in July 2020, when 239 scientists co-signed an invited commentary piece in the journal Clinical Infectious Diseases calling on national and international health and regulatory bodies to "recognize the potential for airborne spread of coronavirus disease 2019." Clashes with the World Health Organization followed. The WHO argued that the science wasn't "definitive" enough and urged further study.
In October, the WHO (and other agencies, like the US CDC) updated transmission advice, stating aerosols could spread COVID-19 in "specific settings" that are poorly ventilated and crowded, such as restaurants or nightclubs. How much infection is caused by aerosol transmission is still an open question, but there is a clear and obvious way to reduce your risk: masks.

WHO technical lead Maria Van Kerkhove speaks at a March 11 press briefing on COVID-19, at which WHO Director-General Tedros Adhanom Ghebreyesus announced that the coronavirus outbreak could be characterized as a pandemic.
We won't relitigate all the arguments against mask wearing here, and it's an area of public health where misinformation has been rampant. The vast majority of scientific research now shows masks are an essential component of the COVID-19 response. Alone, they're not enough, but combined with distancing, hand hygiene, cough etiquette and a range of other measures, they will limit the spread of disease.
Infection via contaminated surfaces was a concern early, with all manner of objects and materials being tested to see how long SARS-CoV-2 would survive on them. Money, packages and door handles were all considered potential hotspots. In May, the CDC specified that this type of transmission was not likely to be "the main way the virus spreads."
What are the symptoms?
SARS-CoV-2 has proven to be a much more canny virus than we predicted. Like previous coronaviruses, it chiefly affects the respiratory tract. Mild symptoms, like a dry cough and a fever occur commonly and can resolve without hospitalization. Some patients will have lethargy and a sore throat.
More severe symptoms see infected individuals experience a shortness of breath and chest pain. The lungs are compromised and become inflamed and the tiny air sacs within fill with fluid. In the most severe cases, patients require mechanical ventilation to assist breathing. These characteristics have been seen since the first cases appeared in Wuhan.
Reports began to surface in March that some coronavirus patients were experiencing anosmia -- a loss of smell. Research has shown the virus is able to enter and impair the activity of specialized cells in the human olfactory system responsible for our sense of smell. Loss of taste has also been reported.
Although the respiratory tract is where SARS-CoV-2 gets a foothold in the body, the virus has far-reaching and long-lasting effects on the human body. "Originally we thought that COVID-19 was primarily a respiratory illness," says Adrian Esterman, an epidemiologist at the University of South Australia. "We now know that it can affect just about every organ, with the potential to cause long-term health problems."
The most severe cases of COVID-19 are characterized by inflammation. "An overexuberant immune response is what wreaks havoc with your body," Labzin says. Some COVID-19 cases see the body's white blood cells produce a lot of cytokines, small proteins that fight infections. They can also recruit more cells to defend against a virus. However, generating too much cytokine can do real damage -- and research has shown an abundance of cytokines can damage the cells lining blood vessels.
This full-body response can even be damaging to the brain. In some patients, blood vessels in the brain are damaged indirectly -- SARS-CoV-2 doesn't necessarily infect brain cells (it may be able to), but the body's overactive immune response can cause the vessels to thin or leak and may result in lasting neurological damage.
Scientists are learning that bodies don't just bounce back to full health after infection. A variety of disparate symptoms seem to stick around long after patients leave the hospital or no longer test positive for the disease. The long-term prognosis for recovery from a COVID-19 infection will be an intense area of study in 2021 as scientists try to understand how negative effects linger in patients known as "long haulers." Sometimes these symptoms last for weeks, other times they are still with patients eight months later -- the impact will only truly come to light as the year progresses.
Is there a treatment for the coronavirus?
A year ago, this section was three sentences long. It called coronaviruses "notoriously hardy organisms" (they are) and stated "we have not developed any reliable treatments or vaccines that can eradicate them" (we hadn't.). By the end of 2020, multiple biotech firms had built vaccines that can protect against coronaviruses, in an incredible feat of scientific research and spirit. "To develop a safe and efficacious vaccine in 12 months is unheard of," Esterman says.
Vaccine rollouts have been occurring across the world. Different candidates, using a variety of different biotechnologies, have been approved for emergency use in places like the US, UK, Canada, Israel and a handful more nations. Many others will approve jabs in the months to come and begin to vaccinate their populations.
The first two vaccines across the finish line are built around mRNA, the instructions cells use to build proteins. The technology has been in development for over two decades, but the pandemic accelerated research into this vaccine strategy.
The vaccines contain a synthetized strand of mRNA that tells human cells to make spike proteins, similar to those on the surface of SARS-CoV-2. The cells oblige, and when the spikes are shown to the immune system, the body's defenses kick into gear. The vaccines then simulate a real infection without the nasty symptoms -- and help provide lasting immunity. If a patient comes into contact with the real coronavirus, the body knows to destroy it before it can cause any harm.

Having coronavirus vaccines approved for emergency use in less than a year is remarkable.
While two mRNA vaccines, from Pfizer/BioNTech and Moderna, have been approved for use, there are still questions over how long they might provide immunity and whether they can stop disease transmission. The data shows they are safe and can prevent severe disease, but do they stop a person from being infected? That's still unclear.
So we're not quite out of the woods -- we're still stuck in a thicket. New variants of the coronavirus have evolved in the past three months, evading some of our immune defenses. Ensuring our vaccines will still be effective against them is one of the major challenges for 2021. Early research looks good, but there are multiple mutations in the new variants that will require further examination.
More vaccines are showing promise, too, with the New York Times' tracker currently showing eight in limited or early use. The Sinopharm vaccine, approved for use in China, has not published results from its Phase III trial but reportedly has an efficacy of around 80%. It uses inactivated pieces of SARS-CoV-2 to generate immunity.
A year on
At the end of the original piece, we linked to a WHO thread on Twitter from Jan. 17, 2020. It provided rudimentary advice on protecting yourself against coronavirus that focused on hand hygiene and respiratory hygiene. Maria Van Kerkhove, from the WHO's emerging diseases unit, recommended washing hands with soap and water and sneezing or coughing into your elbow.
Those recommendations the WHO still stand today. Washing your hands and sneezing into your elbow are extremely important. But we've added additional layers of protection as we've learned more about SARS-CoV-2 and its transmissibility.
Ian Mackay, a virologist at the University of Queensland, highlights these additional layers in the "Swiss Cheese Model" of pandemic defence, an infographic that went viral toward the end of 2020.
The new version as promised (ver2).
— ɪᴀɴ ᴍ. ᴍᴀᴄᴋᴀʏ, ᴘʜᴅ 🦠🤧🧬🥼🦟🧻 (@MackayIM) October 15, 2020
It adds vaccines (at the end because gen1 won't simply fix everything) & tracing has been combined with the fast & sensitive testing slice.
I've combined hand & surface cleaning.
Constructive feedback welcome. pic.twitter.com/mE7LOl7Y2c
"The real power of this infographic," Mackay told the New York Times in December, "is that it's not really about any single layer of protection or the order of them, but about the additive success of using multiple layers, or cheese slices."
We've learned the best ways to defend against COVID-19, but cases continue to rise in many parts of the world. Is it likely we'll be able to control the pandemic in 2021? There's reason for hope, but we need only look at some of 2020's great failures to see how quickly the virus can become unmanageable.
In our second pandemic year, science will continue to probe and refine the answers to these six fundamental questions. And it must. Doing so is critical to prepare for -- or ultimately, to prevent -- the next pandemic.