How eICUs are helping hospitals deal with coronavirus overload
These remote-monitoring facilities were already helping the sickest patients get access to critical-care specialists. COVID-19 has further proved their value.



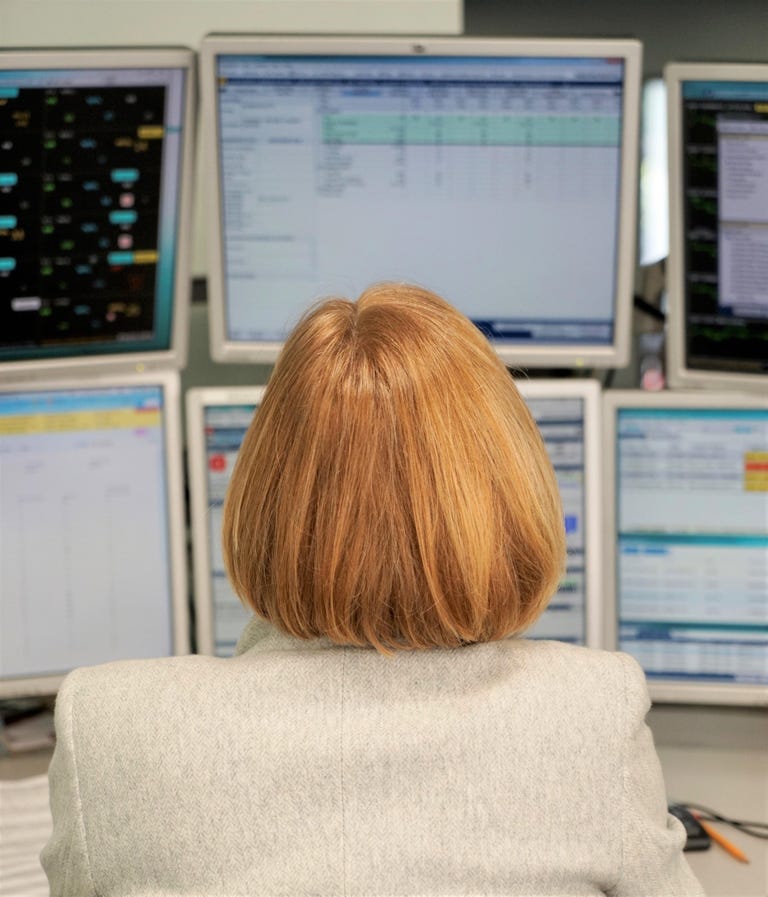
Critical-care nurse Clark Wurth monitors patients remotely from Sutter Health's electronic intensive care unit in downtown San Francisco.
Blink and you'd think nurse Clark Wurth is an air traffic controller. He dons a headset as he sits in front of six huge monitors flashing with alerts and colorful moving charts.
Blink again -- as Wurth zooms in on a COVID-19 patient on a respirator -- and you're transported to a hospital ICU bed. You can make out the smallest details, like the texture of the patient's blanket and the pads placed on her pressure points for when she's turned into the prone position to help increase the amount of oxygen getting to her lungs.
Wurth is caring for the patient, a woman in her late 40s in acute respiratory failure at Sutter Alta Bates Summit Medical Center in Berkeley, California, from 20 miles across the bay, in San Francisco, at one of the Sutter Health medical system's two electronic intensive care units, or eICUs.
He can monitor the patient's vitals, check the medications she's taking, and look at her ventilator settings without having to put on personal protective equipment, save for the face mask required of all California office workers because of the pandemic. The telemonitoring installation includes interactive video and remote diagnostic tools that can access any critical changes in a patient's condition -- and alert Wurth instantly. Bedside, there's a button to push for immediate eICU assistance.
"How does a nurse monitor 50 patients at a time?" asks critical-care doctor Thomas Shaughnessy, who's sharing the shift with Wurth on this late July morning. "The answer is, they have help," he responds, alluding to the telemonitoring system.
Critical-care Nurse Karen LaBerge works from Sutter's eICU in San Francisco, but she also works bedside with patients. The latter, she says, is more "emotionally exhausting."
Shaughnessy, who also happens to be the longtime medical director here at the Sutter Health Bay Area eICU, says the program's goal hasn't changed much since its earliest days back in 2004: making sure the sickest patients at both rural and urban hospitals in its geographically diverse system get access to specially trained nurses and doctors 24 hours a day.
But COVID-19 -- the disease that's caused by the coronavirus and that's been landing massive numbers of patients in ICUs for long stays -- forced Shaughnessy and his colleagues to think creatively to meet that goal. In fact, the coronavirus has forced the medical industry at large to rapidly embrace telemedicine, and the tech that was largely already in place. Sutter's answer to a potential COVID-19 surge came in the form of iPads strategically placed on stands or carts that could be used in converted ICU rooms.
Normally, between the San Francisco and Sacramento eICU hubs, Sutter can care for up to 395 patients, in beds set up with its remote-monitoring installations at its 18 hospitals. With the iPad deployment, and in the case of a COVID-19 surge, it could monitor up to about 600 beds, Shaughnessy says. In late August, about half the patients the two hubs were monitoring -- about 200 patients -- had COVID-19. That was a peak for the hospital system.
COVID-19 'stress test'
Sutter's eICU program was the first of its kind on the West Coast, and one of the first in the US. But other hospitals quickly followed suit as eICUs proved a good solution to a chronic shortage of critical-care doctors in the US. The life of an intensivist, as they're called, can be grueling, since they work nights and weekends. The eICU approach made "lots of sense," says American Telemedicine Association President Joseph Kvedar, especially for hospital systems with "enormous geographic reach."
"How do I take a resource like an ICU clinician and spread them around?" he asks. "Well, technology allows you to do that, and that's what the eICU is all about."
Philips executive Karsten Russell-Wood, whose company supplies hospital systems like Sutter with the eICU, or teleICU remote-monitoring technology, says one of his clients, Emory Healthcare, took the concept of spreading ICU clinicians around one step further -- and farther. Emory assigned critical-care providers to monitor patients in Georgia from an eICU at Royal Perth Hospital in Western Australia.
"All of a sudden, intensivists got to work the daytime in Australia while monitoring patients in Atlanta who had absolutely no idea their physician was far away," Russell-Wood says. "You really get into this imaginative state of, 'Wow, care is anywhere!'"
And that's where 5G, that superfast wireless tech that's just starting to find its place in the world, will come into play. "In health care, what 5G enables is not only improved receptivity and access to data, but it allows that data to be transmitted faster," Russell-Wood adds. He, too, sees an eICU nurse like Wurth as a sort of air traffic controller, with 5G enabling more seamless communication with the critical-care pilots.
"Ultimately, 5G is going to impact the endpoint more than it's going to impact the infrastructure system itself," Russell-Wood says.
eICUs, and telemedicine in general, were already "on the upswing before the pandemic," adds Dr. Amesh Adalja, a senior scholar at Johns Hopkins University Center for Health Security. But COVID-19, with its infection control issues, "is specifically a critical illness that can lend itself well to eICU because we try to limit how many providers go into a room." The eICU doesn't replace bedside staff, but it can supplement them while also keeping the trained intensivists physically removed from potentially infectious patients, he adds.
Dr. Adam Seiver, a longtime medical director for Sutter's Sacramento eICU hub and who also works for Philips, says Sutter's program has gone through three phases. First, in the early 2000s, there was a discovery phase, in which bedside providers had to figure the role the eICU would play. For urban hospitals, it was more of a complementary service, a second set of eyes. But for smaller, remote hospitals, where 24/7 ICU staffing wasn't practical or affordable, the eICU filled a critical void. The second phase, Seiver says, was everyone settling into their established eICU roles.
COVID-19 brought on the third phase, when the eICU "became an absolutely necessary component of being able to respond to surges," he adds. With COVID, "people discovered that the ability to access people remotely applied not only from 300 miles away ... but also from five feet away. We could use our software to not have to go into the room."
COVID-19 has forced patients and clinicians to see the benefits of remote monitoring, adds Philips' Russell-Wood. "I think what we've seen is that every standard of care is being rethought with the concept of stress-testing."
Indeed, in August the Centers for Disease Control published guidance for health care providers on using telehealth to expand services during the COVID-19 pandemic, highlighting improved patient health outcomes as a potential benefit.
Tech support
If you ask Shaughnessy and Bay Area eICU Operations Director Lisa Ochoa what tech innovation has been the most transformative for their program, the answer is clear: the electronic health record, or EHR, which is a collection of patient health information in digital format that can be shared across different health care settings. EHR adoption got a boost with a 2009 law that offered financial incentives, and most hospitals had embraced them by 2015.
Shaughnessy recalls the days prior to EHRs, when hospitals had "rooms filled with file cabinets." He says those days were "like driving a sports car in first gear." With EHRs, he says, productivity tripled.
Kvedar agrees that electronic records have had a huge impact, but he also offers a nod to everyday consumer tech like better bandwidth, high-definition cameras and even how cheap LCDs have become.

Dr. Thomas Shaughnessy, medical director of Sutter's Bay Area eICU, uses FaceTime on his iPhone to touch base with a bedside nurse.
"There's been no leapfrog in any particular space that helped us do this 1,000-fold differently," he adds. "It's just things have gotten gradually less expensive, more connected and more powerful."
Video chat products like Apple's FaceTime, along with Wi-Fi improvements, have also been key to creating makeshift eICU rooms and even getting closeups on a wound -- though Seiver says he usually prefers the fixed cameras on the wall to a shaky one held by a nurse.
But the real power of the eICU, Seiver explains, is its role as a "central cognitive clearing house." Particularly for something like a novel virus, where there's a lot of speculation and new information that needs to be learned on the fly, "it's a way to quickly standardize or at least communicate approaches to care that otherwise might not spread as quickly," he says. One example Seiver mentions is spreading the word about the proning technique used on the Berkeley patient in respiratory failure.
As for the eICU software, Russell-Wood says Philips is constantly adding smart algorithms and AI-enabled tools to leverage medical data so that clinicians can make informed decisions. Predictive analytics allows clinicians to be proactive rather than reactive, he adds. "You can actually predict adverse events simply by recognizing adverse trends that the system is telling you to look at."
Of course, technology comes with costs -- and eICUs are pricey: An article in The Permanente Journal estimates it costs $2 million to $5 million just to build the "command center" for an eICU. The article also estimates startup costs at between $50,000 and $100,000 per bed. The makeshift, iPad-enabled eICU beds are much cheaper. Still, cost is a source of tension.
"For the 17 years that eICU has been present at Sutter, there's always been constant pressure to demonstrate cost-effectiveness," Seiver says.
And the eICU's success is almost impossible to measure, he adds, though there's lots of trying. Statistics from Sutter and Philips show how eICUs have shortened the length of ICU stays, reduced operational costs per patient stay and reduced mortality rates.
Or you could simply look to that COVID-19 patient Wurth was caring for. She's out of the ICU and recovering nicely.
