
How the delta variant breached Australia's COVID fortress
Australia was a pandemic success story, but it has been overwhelmed by the delta variant. What happened?


The first case drove limousines. The man, in his 60s, ferried international airline crews from Sydney Airport to hotel rooms, where they quarantined before jetting off on their next flight. While transporting one of these crews — possibly three people from a FedEx freight plane — the driver unwittingly came in contact with the coronavirus. He had not been vaccinated.
On June 16, he tested positive for COVID-19. The virus had invaded his lungs several days earlier. Genetic testing showed the strain he harbored was unlike any previously seen in Australia: the delta variant, which had ravaged India during the opening months of 2021 and was rapidly becoming the dominant strain across the world.
Within hours of testing positive, the driver's wife had also returned a positive test. One positive became two. This was expected. Delta is highly transmissible. Close contact with infected individuals carrying the variant all but ensures the virus will hop between human hosts.
While unknowingly infectious, the man had visited a large shopping mall within walking distance of Sydney's famous Bondi Beach, as well as a nearby cafe. Contact tracers, who had so effectively helped to arrest Australia's first wave, began to ring alarm bells.
In these bustling locations, delta found its chance to slip through Australia's defenses. The island nation had long been held up as a pandemic success story, keeping the virus at bay with some of the strictest preventive measures in the world. Those measures had quashed outbreaks or outright prevented them, allowing the country to live relatively free and open while the virus raged overseas.
Delta flipped the script. It exposed ineptitude and complacency among the country's political leaders and uncovered a creeping pandemic fatigue that had infected the population. It divided Australia's most populous states and showed how quickly the health response can unravel in an unvaccinated country because of poor communication and rising levels of vaccine hesitancy.
By the end of June, Sydney, the capital of the state of New South Wales, faced a worrying outbreak. As cases began to emerge across the city, NSW leader Gladys Berejiklian labeled the outbreak "the scariest period" in the state's battle against the coronavirus. By June 26, just 10 days after the limousine driver's positive test, there was only one option.
Sydney headed into lockdown.

Bondi beach in December 2020.
Built different
Australia has been a near-impenetrable fortress during the pandemic. Stringent quarantine rules have seen all international arrivals isolate for 14 days, at their expense, in converted hotels, sometimes under police guard. As a result, coronavirus incursions have been uncommon.
But the virus has found fissures in the fortress. Occasionally, it has broken through the country's "leaky" quarantine system, hitching a ride in unvaccinated lungs and slipping containment by riding cross-city with hotel cleaning, security and transport staff — like the limousine driver. Other times, quarantined travelers have been exposed to airborne viral particles as they moved between poorly ventilated hotel suites.
In mid-2020, the southeastern state of Victoria entered a lockdown that lasted for 112 days as a result of the "classic" coronavirus strain, genetically similar to the one first found in Wuhan, China. But the delta variant that rapidly spread through Sydney in July 2021 is built different. Experts have dubbed it the "most formidable version" of the virus yet.
"In the lab, it doesn't look much different to the other variants," says Stuart Turville, an immunovirologist at the University of New South Wales in Sydney. "But in the wild it is certainly causing havoc."
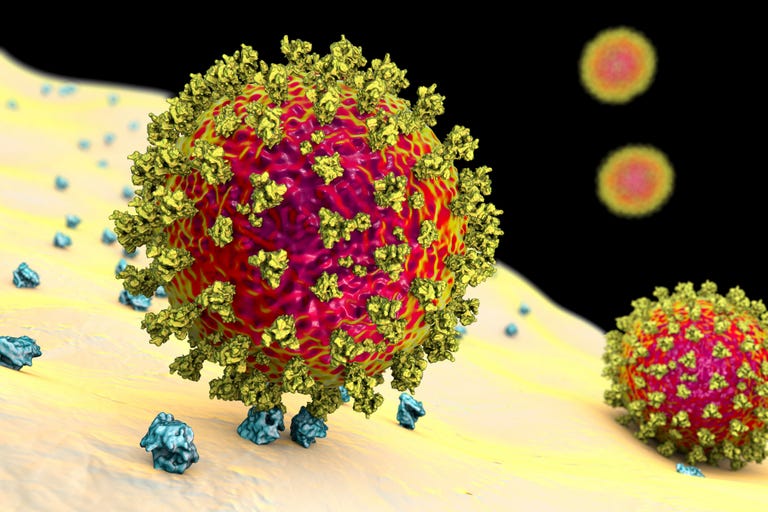
The coronavirus enters human cells by using its spike to grab onto the ACE2 receptor, pictured here in blue.
Just like the classic strain, delta has to latch on to human cells to hijack them and produce more copies of itself. The ball-shaped virus does this by using its spike protein, a club-shaped appendage that protrudes from its body. The spike snags on a receptor known as ACE2, naturally present on human cells. This is like a lock on a vault door; the spike is the virus' skeleton key, facilitating entry into the cell.
Delta has mutated in such a way that its spike is better than that of previous strains at latching on to ACE2 and entering cells — and it doesn't alert the human immune system as readily.
"It seems to have an invisible immune shield that means it doesn't trigger a strong immune response," says Nikolai Petrovsky, a professor of medicine at Flinders University and founder of vaccine developer Vaxine, currently trialing its own COVID jab.
Delta also seems to make a lot more particles, reproducing with an intensity and speed unmatched by earlier forms of the virus. One study, yet to be peer-reviewed, looked at delta variant cases in China and reported viral loads "1,000 times higher" than original strains from early 2020. Viral load is an indirect measure of how much virus is in the body. It's a simple numbers game: the higher the load, the more you can pass on.
Breaching the fortress
A month after the Sydney limousine driver tested positive, daily case numbers in NSW topped 100. A few weeks later, 300. Then 400. Then 600. A stark rise in hospitalizations followed. In global terms, the numbers may seem tiny. For Australia, they'd not been seen for almost a year. How did it come to this?
As the pandemic was defeating America in 2020, Australia was mostly living free. Much of the population was spared long lockdowns through a combination of aggressive border controls, a little luck and a public willingness to mask up and just get on with it. Australians listened to health experts and stayed home when instructed to.
But when Sydney confronted delta in June 2021, a different feeling descended on the city.
Before lockdown, cases had hovered at zero for months. Masks had become an increasingly uncommon sight; posters for social distancing restrictions hung in windows, but if you looked through the glass, those warnings were mostly ignored. Living without the virus for so long had allowed a creeping complacency to infect the state — a complacency delta had mutated to exploit.
After squashing the curve in early 2020, Berejiklian, the NSW state leader, was splashed over the front of national newspapers and in one notorious profile labeled as "the woman who saved Australia." She wasn't shy about congratulating the state for keeping the virus at bay. She lauded her pandemic response, contact tracing and avoidance of lockdowns as "the gold standard."
“The Woman Who Saved Australia” @FinancialReview writes of @GladysB pic.twitter.com/jpLltiQ0g5
— Andrew Greene (@AndrewBGreene) April 29, 2021
Things unraveled when delta catapulted over the walls of Fortress Australia.
The state government lumbered along, seemingly ignoring the possibility the variant had slipped through the cracks and spread insidiously through the community. The limousine driver's age should have seen him vaccinated as part of the government's rollout, but he wasn't. The valiant efforts of contact tracers were not enough to keep up with the spread. The outbreak spun out of control. Berejiklian's gold standard turned to lead. The initial two-week lockdown order stretched out to five weeks, then nine.
This was predictable. "New South Wales went into lockdown on day 10, probably a week too late," says Adrian Esterman, an epidemiologist at the University of South Australia. Modeling has shown that for every three days a lockdown is delayed, three weeks can be added to the end date.
Berejiklian remarked that "delta is very different to anything we have seen before" and the state couldn't have prepared for it. But while it is more infectious, experts suggest it shouldn't change how we combat COVID-19, just how quickly and aggressively we do so. "The same measures that worked last year will work against this variant as well, we just have to do them better, faster," says Mike Toole, an epidemiologist at the Burnet Institute in Victoria, Australia.
Other states in Australia that had to contend with delta acted aggressively. South Australia and Victoria both entered lockdown within four days of detecting the variant. The latter had learned a lesson in 2020: Go hard, go fast. The New South Wales government, hellbent on living open and free, didn't learn the same lesson.
In an unvaccinated population, that decision would prove disastrous.
Apples and oranges
With vaccines so critical to combating delta, there was little Australia could do but lock down when it arrived. Before the delta outbreak the pace of vaccination was remarkably slow. Prime Minister Scott Morrison insisted that getting people vaccinated was "not a race," and the country's vaccination rate languished, the worst in OECD countries, with just over one in six people fully vaccinated by late June. The comments would come back to haunt Morrison as the rollout became increasingly complicated due to complacency, fear, confusion and politicking — with the brunt borne by one vaccine in particular: the Oxford-AstraZeneca vaccine.
Though this vaccine had proven safe and effective around the world and had helped the UK out of its pandemic hole, it had a nightmarish run in Australia.
The vaccine, which uses a modified chimpanzee virus to produce immunity against COVID-19, blitzed through clinical trials in 2020, showing high levels of effectiveness against original strains of the virus. Its successes led the Australian government to pick it as the vaccine of choice, announcing it would be manufactured locally and ensuring it would form the backbone of the nation's vaccination strategy in the first half of 2021. The Pfizer mRNA vaccine was also greenlit for use in Australia and would be shipped into the country, with an initial order of 10 million doses.
Early data from AstraZeneca's clinical trials came via a press release and showed the vaccine was around 79% efficacious against disease. But scientists and the press were quick to critique it, accusing the company of presenting data in a misleading way. The critique was justified, but it came just weeks after Pfizer released its first results, citing over 90% efficacy. At the time, Daniel Altmann, an immunologist at Imperial College London, told Nature: "We're slightly in danger of rushing to compare apples and oranges ... [t]here's a long, long way to go before these data settle down and get reported and published in full."
But it was already too late. The hyperspeed news cycle ensured the Pfizer apple would be pitted against the AstraZeneca orange.
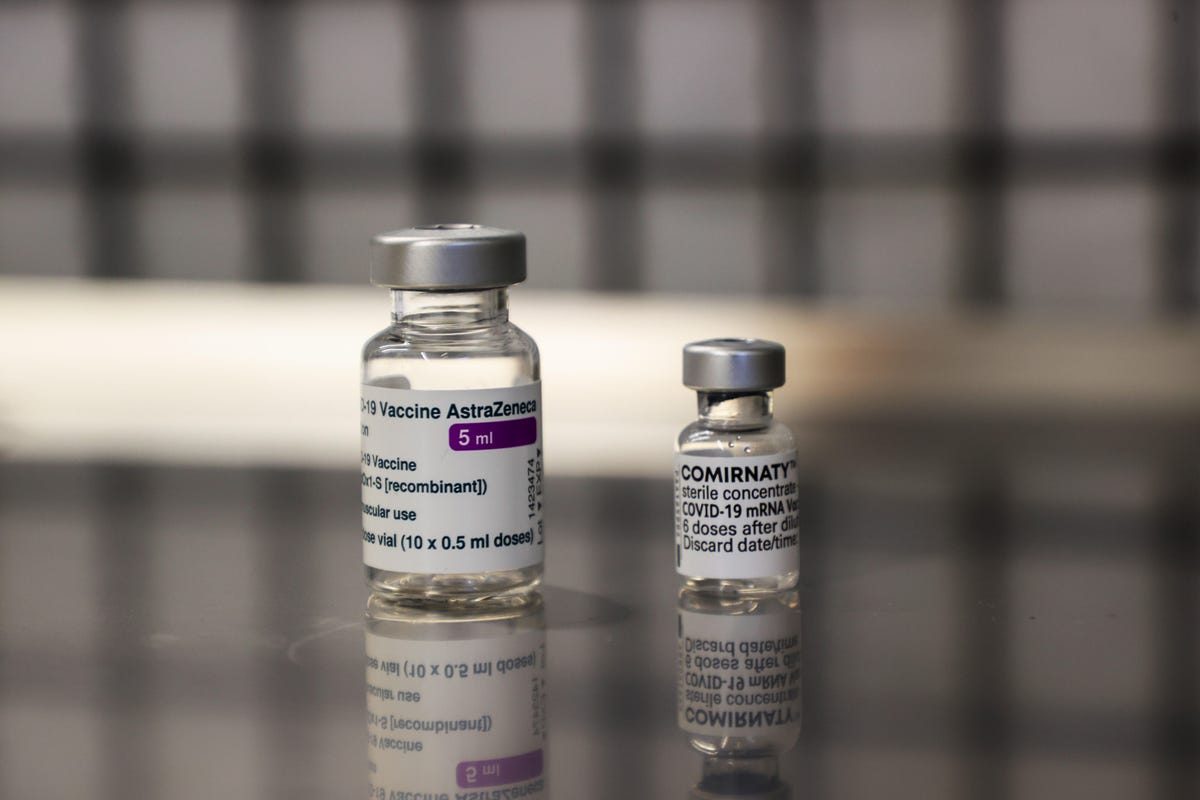
Australia's first two vaccine options, AstraZeneca and Pfizer, were constantly pitted against each other in the media.
The Australian Broadcasting Corporation ran a segment in January 2021 on the vaccine strategy Australia was using, about a month before AstraZeneca had been approved by the country's chief regulatory body. The first voice in the segment was Raina MacIntyre, an epidemiologist at the University of New South Wales, and her assessment was damning. "If we go ahead with the AstraZeneca vaccine, we'll be likely living with the virus for a very long time," she said.
Hesitancy around AstraZeneca had been festering on social media and quietly throughout the country, and this type of definitive statement only served to increase it. Science communicators were right to point out the differences, but the nuance was lost: AstraZeneca was quickly labeled an also-ran that couldn't compete with Pfizer.
Confidence in AstraZeneca fell further once scientists linked it to an extremely rare but potentially fatal clotting disorder. In March, a handful of European countries, including Austria, Germany and Denmark, paused their AstraZeneca rollouts as reports of clots rolled in. Fear, and misinformation, began to spread. The complex, confusing talk about risks and benefits muddied the picture on AstraZeneca even more.
In Australia, every post-vaccination death became front-page news. "All we heard about was blood clots," says Nathan Bartlett, a viral immunologist at the University of Newcastle.
When delta arrived and spread out of control, the same experts who had diminished AstraZeneca began emphasizing the importance of being vaccinated. Health officials were offering different opinions on who should get what vaccine and when. The to-ing and fro-ing saw experts face off publicly, creating a new uncertainty and doubt about the vaccine.
Australians older than 60, scheduled to receive AstraZeneca, wanted to wait for Pfizer, while those younger than 40 weren't provided access to vaccines at all, even as they cried out for them. When young Australians wanted to get AstraZeneca, they were told by some public health officials to speak to their GP first and by others that it wouldn't be available at all. Pfizer demand soared, but the Australian government hadn't been able to acquire adequate supplies. The rollout stumbled, then appeared to stall. Millions of AstraZeneca vaccines were going unused.
"We could quite easily accelerate the rollout of the vaccines if people would take AstraZeneca," Toole told me in late July. "But I think it might be a lost cause now."

Eligible Australians have shown a reluctance to receive the AstraZeneca vaccine.
Open windows
Even in the face of more infectious and stealthy variants like delta, vaccines still provide the best protection against severe disease. The genetic tweaks present in delta's genetic code blunt some of the vaccine's protective effects, but don't erase them.
In July, researchers demonstrated that one dose of the Pfizer or AstraZeneca vaccines provides low protection against infection — but two doses remained a powerful way to prevent symptomatic disease. Russia's Sputnik-V, among other vaccines, has been shown to be "around 83% effective," according to Health Minister Mikhail Murashko. It's less clear how China's homegrown vaccines fare against the variant.
More optimistically, data from Canada, Scotland, the US and the UK has begun to show that while vaccinated individuals can be infected, they seem less likely to end up in hospital or die. Further research, by Australia's Doherty Institute, strengthened these claims. The message should be clear, notes Jill Carr, a virologist at Flinders University in Australia. "Protect yourself against COVID-19, irrespective of what variant it is," she says.
But delta is proving unstoppable, even in places with high vaccination rates.
Despite half of its population being fully vaccinated, the US has seen a surge in daily COVID-19 cases. Over 90% of all new cases are of the highly transmissible variant. Hospitalizations are rising, overwhelmingly in unvaccinated individuals, with some reports stating that 90% to 95% of those who end up in hospital hadn't received a vaccine.
Experts have long warned that the coronavirus will continue to evolve and mutate. The virus is in constant battle with our immune systems, changing its genetic code in ways that help it hide from immune cells. Six months into the pandemic, Bruce Thompson, a respiratory expert at Swinburne University in Australia, told me it was likely we'd be living with this pandemic through to 2022.
Australia's delta outbreak reveals what happens when a new variant collides with a massively undervaccinated population. Without lockdowns, delta would be causing the worst surge of the pandemic yet.
The frustrating thing for many Australians is that it didn't have to be this way. "We had a window where we could have gotten a large proportion of the eligible population vaccinated and we didn't take it," Bartlett says. The same story has been true of pandemic success stories like South Korea and Vietnam. Having inadequately protected their populations when cases were low, they now face a resurgent virus finding cracks in their defenses.
In other parts of the world, the situation is even more dire.
Left behind
On Aug. 18, daily coronavirus cases in Sydney reached a record high of 633, despite seven weeks of lockdown. Hiding within the numbers was a stark and worrying reminder about how this virus exploits inequalities.
Inequality plagued the pandemic response across the world long before the first vaccines began to roll out. While high income earners easily moved to home offices, low-paid workers in essential services couldn't make the same transition. That meant they were more likely to come into contact with infected individuals at work. Other industries, like hospitality and tourism, shut down for good, leaving many without income at all.
Delta, spreading faster than any previous variant, was always going to widen the chasm.
This is true of Sydney's outbreak. The southwest, where the majority of cases were being detected, is home to a large proportion of disadvantaged communities and migrant populations who speak English as a second language.
Health messaging wasn't tailored to inform these populations as cases began increasing. An exposé by the Australian Broadcasting Corporation showed the federal government's messaging was out of date by two months. The whirlwind of conflicting guidance about quarantine, vaccines and movement restrictions only exacerbated confusion. In addition, without financial assistance from the government, those in the southwest had to continue working in essential services, sometimes contracted to clean or deliver goods across the city without the ability to take sick leave. Combined with low levels of vaccination, their vulnerabilities lay bare.
As the virus started to spread outside Sydney's inner suburbs, regional Indigenous populations began to see a surge in cases. The opposition government warned these communities were at particularly high risk because only around 15% of Indigenous Australians are vaccinated compared with the nation's 26% total.
Put simply, these communities were left behind.
The problem extends beyond Australia's borders. As unvaccinated hospitalizations and deaths began to shoot upward in the US this past July, Rochelle Walensky, director of the Centers for Disease Control and Prevention, said the US is now facing "a pandemic of the unvaccinated."
"The unvaccinated" make up the majority of people on the planet, with less than 25% having received two doses of a vaccine. In low-income countries, the situation is alarming, with just over 1% receiving a single dose of vaccine. Those nations, too, are being left behind.
The myopia threatens all the hard-fought wins of the past 20 months. Modeling, published in the journal Science on Aug. 17, showed that redistributing surplus vaccine from high-income to low-income nations is "likely advantageous" at preventing new variants from arising. Scientists and the World Health Organization have consistently urged the world to donate vaccines to the COVAX program, a vaccine-sharing scheme that delivers vaccines to countries that cannot afford them. With a more transmissible and potentially more deadly variant, it's low-income nations that are the most exposed.
"We're on track for the second year of this pandemic to be far more deadly than the first," Tedros Adhanom Ghebreyesus, director-general of the WHO, warned in May.
Against this backdrop, the resurgence of delta in Australia becomes a window into one possible future. If new variants emerge in undervaccinated places across the globe, experts are concerned we might be sent spiraling back to the very early days of the pandemic, where hospitals are overwhelmed, more lives are lost and lockdowns once again become commonplace.
Without vaccinating the world, "the monster's going to appear in another setting," says Catherine Bennett, chair in epidemiology at Deakin University in Australia.
"Even if we reduce our chances of developing variants here, we'll get that variant that comes back to haunt us if we don't partner with other countries to make sure we're assisting the global rollout."
Beat delta back
A multitude of factors have conspired to make this Australia's worst outbreak yet: A leaky quarantine system, botched vaccine rollout and the Australian government's constantly shifting vaccination targets put the country in a bad position to defend against delta. Inaction by New South Wales' leadership exacerbated this, alongside a complacency born of months of low case numbers and pandemic fatigue. Delta is concerning. It's complicated our path out of the pandemic. But it cannot be an excuse.
Fortunately, seven weeks after it first breached Fortress Australia, there's been a gradual shift in understanding: We're not helpless against the variant — but we must redouble our efforts.
Two Australian cities provided a blueprint for beating delta back. The town of Adelaide locked down within three days and saw delta disappear. Queensland, home to the nation's third-most populous city, curtailed rising case numbers within weeks. Similar stories of aggressive containment have been seen across the country. Victoria jumped on its delta outbreak within days and the nation's capital territory, without a case for 104 days, went into lockdown for a week after a single positive was found on Aug. 12.
Those states learned the lesson: Without vaccines, you need to go hard and fast.

COVID-19 vaccine pop-up clinics, like this one at the Lebanese Muslim Association in Sydney's southwestern suburb of Lakemba, have become more common as the state battles the worst outbreak since the pandemic began.
The AstraZeneca hesitancy that punctuated the Australian rollout has been gradually dismantled by a renewed urgency. The population has been spurred into action, with the pace of vaccination in New South Wales exploding, particularly in the vulnerable elderly population. Young Australians, finally given access to the vaccine, have come out in droves to get protected.
Delta has realigned our understanding of vaccination, too. The idea that vaccines will help "end" the pandemic holds, but looking back, the message was a confusing one. Vaccines are unlikely to eliminate the virus from circulation, especially if delta is our new baseline. "We were never expecting to eradicate the virus," says Bennett. "We hoped, at different times, but we never had any indication that we were going to get there."
What vaccines allow for is a level of control over the coronavirus that prevents hospitalizations and deaths from soaring. New vaccines and therapeutics are on their way, likely to help stymie the virus even more. The biggest challenge is to take what we've learned — from the first waves, the second waves, about vaccines, social inequalities and communication — and prevent the next variant from sending us back to square one.
Those learnings are critical if we are to ensure that one unvaccinated limousine driver, just trying to do his job, can no longer unwittingly kickstart an outbreak.